

4 simple poo tests to save your gut
One sample. Four big answers. I can order all of them.

Patients laugh when I bring it up.
But poo is one of the most useful non-invasive tests in medicine.
One sample can tell us if you’re bleeding internally. If your bowel is inflamed. If a bug is causing your reflux. If your pancreas has stopped pulling its weight.
Four tests. Four big answers. Most are simple, cheap, and your GP can order them.
Let me walk you through them.
You can check out my full Substack here
Disclaimer: Come on now….if you notice any change in your bowels, don’t sit on it. Speak to a professional and get your 💩 tested for quick, non-invasive results
1. qFIT (Quantitative Faecal Immunochemical Test)
The qFIT looks for invisible blood in your stool. Specifically, human haemoglobin from the lower bowel.
Why does that matter?
Bowel cancer tends to bleed before it causes pain. By the time you’re symptomatic, the tumour has had a head start.
This is the test the NHS posts through your door every two years.
Welcome to the Bowel Cancer Screening Programme (BCSP).
Adults aged 50 to 74 in England, Scotland and Wales get a kit. Take a tiny sample. Pop it in the post. Results in a couple of weeks.
A positive result triggers an invitation for colonoscopy.
This simple poo test picks up thousands of cancers and many many more high risk polyps (most can be removed endoscopically!)
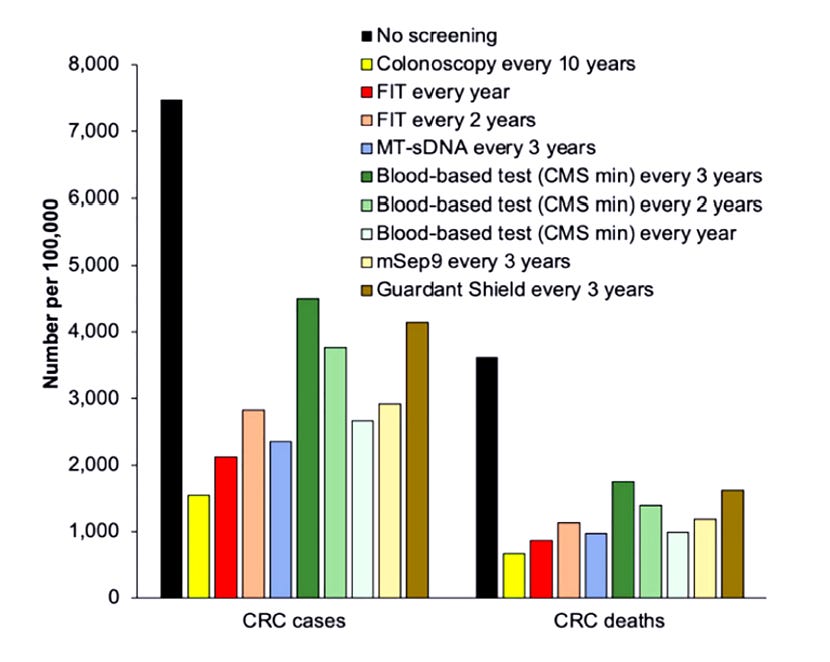
The COLONPREV trial randomised over 57,000 adults to FIT or colonoscopy. FIT detected similar numbers of cancers and was far less invasive. Long-term FIT-based programmes reduce colorectal cancer mortality. Full stop.
For my US readers: you tend to lead with colonoscopy, but the American College of Gastroenterology recommends annual FIT as a perfectly valid alternative for average-risk adults who’d rather not start with a scope. The test still applies.
Got a kit sat in a drawer? Find it. Do it. Send it back.
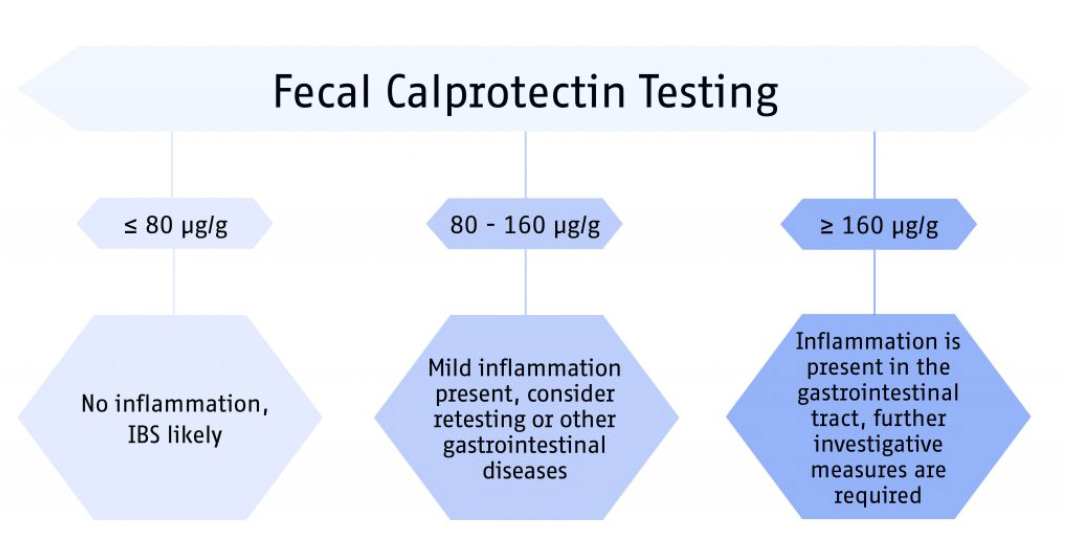
2. Faecal Calprotectin
Calprotectin is a protein released by neutrophils….the white blood cells that flood into your gut when it’s inflamed.
More inflammation, more calprotectin. Simple as that.
Why is it useful? Because IBS and IBD can look identical from the outside. Bloating. Pain. Loose stools. Urgency. The symptoms overlap. The treatments don’t.
IBS (irritable bowel syndrome) is functional. The bowel looks normal but behaves badly.
IBD (inflammatory bowel disease, ie Crohn’s and ulcerative colitis) is structural. The bowel is genuinely inflamed.
Faecal calprotectin separates the two with impressive accuracy.
A landmark meta-analysis (2010) reported a pooled sensitivity of 93% and specificity of 96% in adults at the 50 µg/g cut-off.
NICE diagnostic guidance DG11 recommends it in primary care to help distinguish IBD from IBS. Most UK labs use 50 µg/g or 100 µg/g as the action threshold.
Sensitive? Yes. Specific? Less so. Calprotectin can also rise with bowel infections, NSAIDs, coeliac disease and bowel cancer. A positive test rarely closes the case on its own. It just tells you further investigations are needed!
Practical translation: a high faecal calprotectin usually means a colonoscopy is on the way.
A normal calprotectin in someone with IBS-type symptoms is genuinely reassuring. It makes IBD highly unlikely.
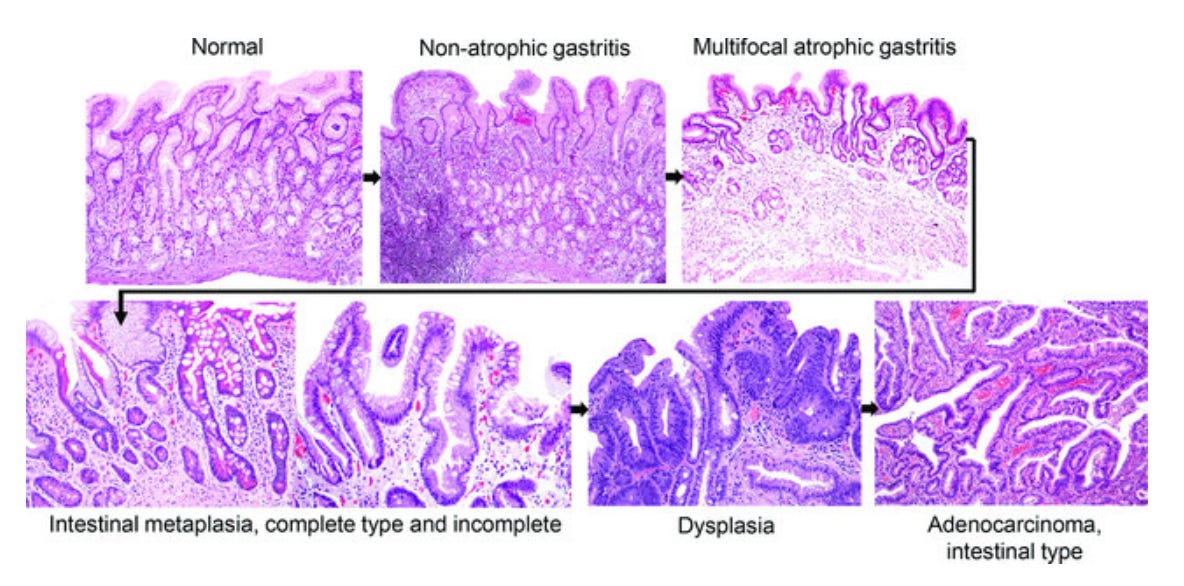
3. Helicobacter pylori Stool Antigen
Persistent reflux? Burning pain in the upper belly? Indigestion that won’t shift?
A bacterium might be the cause.
Helicobacter pylori is a spiral-shaped bug that lives in the stomach lining.
It infects roughly half the world’s population. Most people never know they have it. Some develop gastritis. Some develop peptic ulcers. A small minority develop gastric cancer.
The IARC (International Agency for Research on Cancer) classifies H. pylori as a Class 1 carcinogen. It sits alongside tobacco and processed meat.
Marshall and Warren won the 2005 Nobel Prize for proving H. pylori causes ulcers. Marshall famously drank a culture of the bug to make his point. Reader, he developed gastritis. Hero. I wrote about this story more HERE
The stool antigen test detects H. pylori proteins shed in your poo. Monoclonal versions achieve sensitivity and specificity around 95%, comparable to the urea breath test.
The Maastricht VI/Florence consensus places stool antigen and breath testing on equal footing for diagnosis.
UK NICE CG184 recommends testing for H. pylori in anyone with persistent dyspepsia. If positive, eradicate it with a week of two antibiotics plus a proton pump inhibitor.
For my US readers: H. pylori prevalence in American adults sits around 30 to 40%, higher in some communities. The test is just as useful there.
Been on a PPI for years and never tested? Consider this your sign.
4. Faecal Elastase-1
Stools that float. Stick to the bowl. Leave an oily film. Smell unusually awful.
That’s steatorrhoea. Fat in your poo. The clue points upstream….to your pancreas.
Your pancreas makes the digestive enzymes that break down fat, protein and carbohydrate (lipase, amylase, proteases). When it underperforms, fat passes through undigested and stools become floating, oily disasters. This is exocrine pancreatic insufficiency (EPI).
Common causes:
Chronic pancreatitis (by far the most common)
Pancreatic cancer
Previous pancreatic surgery (eg a Whipple’s)
Cystic fibrosis
Type 3c diabetes
Long-standing coeliac disease

Faecal elastase-1 measures the amount of pancreatic elastase in your stool. The enzyme is made by the pancreas, survives intestinal transit, and arrives in your poo essentially unchanged. Brilliantly simple.
The reference ranges:
Above 200 µg/g: normal
100 to 200 µg/g: mild to moderate insufficiency
Below 100 µg/g: severe insufficiency
The test works best for moderate to severe disease. It can miss milder cases. Watery stools dilute the enzyme and produce falsely low results, so a formed sample is best. The British Society of Gastroenterology recommends faecal elastase-1 as the first-line test for suspected EPI.
When it’s low, treatment is refreshingly simple. Pancreatic enzyme replacement therapy (PERT, brand names like Creon). Take with every meal. Symptoms settle. Weight stabilises. Fat-soluble vitamins recover.
I have written about this topic in detail HERE
Wrapping up
Four tests. One sample. Plenty of answers.
Your gut leaves clues every day. We just need to look. Persistent bleeding, bloating, reflux, weight loss or oily stools? Don’t ignore them. A simple poo test may be all that stands between you and a diagnosis.
Speak to your GP or my secretary! Ask about the test that fits your symptoms.
Struggling with liver or digestive issues that affect your daily life? Invest in your gut health with a private, personalised consultation where I will explore your specific symptoms and develop a targeted treatment plan. Take the first step toward digestive wellness today: https://bucksgastroenterology.co.uk/book-an-appointment/ (I offer both in person and video consultations!)
You can check out my full Substack here
References
van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ. 2010 Jul 15;341:c3369.
Waugh N, Cummins E, Royle P, et al. Faecal calprotectin testing for differentiating amongst inflammatory and non-inflammatory bowel diseases: systematic review and economic evaluation. Health Technol Assess. 2013 Nov;17(55):1-211.
National Institute for Health and Care Excellence. Faecal calprotectin diagnostic tests for inflammatory diseases of the bowel. NICE Diagnostics Guidance DG11. 2013.
Turvill J, et al. Evaluation of the clinical and cost-effectiveness of the York Faecal Calprotectin Care Pathway. Frontline Gastroenterol. 2018 Oct;9(4):285-294.
Quintero E, Castells A, Bujanda L, et al. Colonoscopy versus faecal immunochemical testing in colorectal-cancer screening (COLONPREV). N Engl J Med. 2012 Feb 23;366(8):697-706.
Li SJ, et al. Impact of changes to the interscreening interval and faecal immunochemical test threshold in the national bowel cancer screening programme in England: results from the FIT pilot study. Br J Cancer. 2022 Oct;127:1525-1533.
Gisbert JP, de la Morena F, Abraira V. Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: a systematic review and meta-analysis. Am J Gastroenterol. 2006 Aug;101(8):1921-1930.
Malfertheiner P, Megraud F, Rokkas T, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022 Sep;71(9):1724-1762.
National Institute for Health and Care Excellence. Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management. NICE Clinical Guideline CG184. 2014 (updated 2019).
International Agency for Research on Cancer. Schistosomes, liver flukes and Helicobacter pylori. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Vol 61. 1994.
Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984 Jun 16;1(8390):1311-1315.
Phillips ME, Hopper AD, Leeds JS, et al. Consensus for the management of pancreatic exocrine insufficiency: UK practical guidelines. BMJ Open Gastroenterol. 2021;8:e000643.
Löser C, Möllgaard A, Fölsch UR. Faecal elastase 1: a novel, highly sensitive, and specific tubeless pancreatic function test. Gut. 1996 Oct;39(4):580-586.
Lam KW, Leeds J. How to manage: patient with a low faecal elastase. Frontline Gastroenterol. 2021 Jan;12(1):67-73.
General Disclaimer
Please note that the opinions expressed here are those of Dr Hussenbux and do not necessarily reflect the positions of Buckinghamshire Healthcare NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you. Thank you to the amazing photographers from Unsplash where I get most of my images from.
It's weird how much I enjoy the posts from your group. Thank you. Both my daughter and my late husband have/had celiac disease (I am in the USA). My husband also had AL amyloidosis which affected his gut motility and blood supply (among many other organs). So, frequent discussions about poo.
I would love some advice on how to get my 26 year old daughter to see a gastro doctor. She has bowel anxiety due to urgency and accidents, but I cannot get her to a doctor. She follows a very strict gluten free diet.
Thank you!