

You have a Hiatus hernia - now what?
A structural issue that may not need your attention

“What can you do for my hiatus hernia??” Mr G asked as he walked into the consultation room with me.
He underwent a straight to test (STT for short) gastroscopy; i.e. his GP referred him to his local gastroenterology service who triaged him straight to a gastroscopy (without seeing a clinician) for mild reflux.
The gastroscopy revealed a 2cm hiatus hernia.
He was discharged back to his GP. During the process, he never spoke to a specialist…
Understandably the gastroscopy report led to unanswered questions.
“How are you feeling now?”
“Fine to be honest…..” he replied.
Sadly, a pill can’t fix a hiatus hernia…but an operation is not always the answer either.
Here is what you need to know in less than 5 minutes.
Disclaimer: Hiatus hernias come in all shape, sizes and associated symptoms. This is a general guide. For specific questions, you should ask your healthcare professional.
What is a hiatus hernia?
Your diaphragm is a dome of muscle separating chest from abdomen. It has a small opening called the hiatus. The oesophagus passes through it to meet the stomach. Normally, this opening is snug. About 18mm across.
In a hiatus hernia, part of the stomach pushes up through that gap into the chest cavity. The opening stretches and the anatomy shifts.
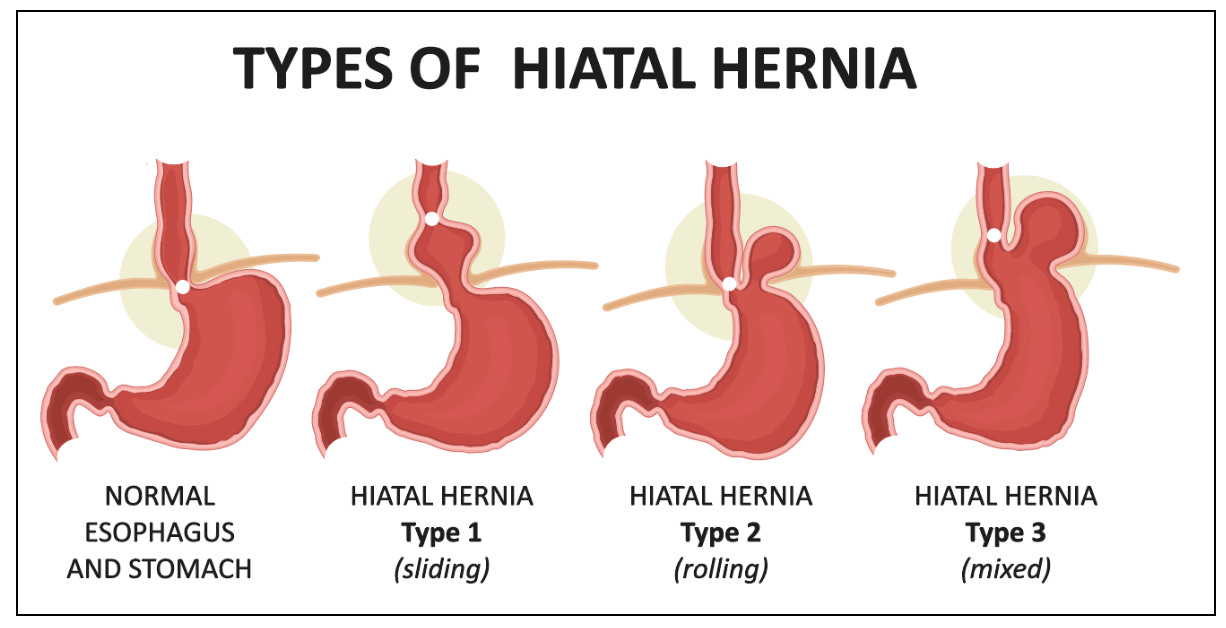
There are four types:
Type I (Sliding) - The junction between oesophagus and stomach slides upward. This accounts for roughly 95% of all hiatus hernias. The most common. Often the least dramatic.
Type II (Para-oesophageal) - The stomach’s fundus (the top portion) herniates alongside the oesophagus, while the junction stays put. Rarer. Around 4-5%.
Type III (Mixed) - A combination of both. The junction and fundus migrate upward.
Type IV (Complex) - A large defect. Other organs; colon, spleen, even pancreas, can herniate through. Thankfully uncommon.
Size matters too. We typically describe them as small (under 3cm), large (over 5cm), or giant (more than 30% of the stomach sitting in the chest). The bigger the hernia, the more likely it is to cause trouble.
Symptoms…..or the lack of them
Most people don’t know they have a hiatus hernia!
Studies suggest around 60% of adults over 60 have some degree of hiatus hernia. Yet only about 9% experience symptoms. The vast majority are symptom free!
When symptoms do appear, they typically involve reflux: heartburn, regurgitation, that sour taste at the back of the throat. Some people experience chest pain, difficulty swallowing, or a feeling of fullness after small meals.
Larger hernias tend to cause more problems. A study of 75 patients found those with hernias over 5cm had significantly more heartburn and acid regurgitation than those with smaller ones. Size correlates with severity.
But a small hernia can cause misery. And a large one can cause nothing at all.
Make it make sense!
Long-term risks
Most hiatus hernias are don’t cause any long term issues.
But complications can occur…particularly with larger or para-oesophageal types.
Cameron lesions - Linear erosions at the diaphragmatic pinch point. They can cause slow, chronic bleeding. In large hernias (over 5cm), these occur in about 13% of patients. The result? Iron deficiency anaemia. Around 30% of people with para-oesophageal hernias have anaemia as a presenting feature.
Strangulation - Rare but serious. Part of the herniated stomach loses its blood supply. The annual risk for para-oesophageal hernias is roughly 1.2%. Small, but not negligible over a lifetime.
Gastric volvulus - The stomach twists on itself. A surgical emergency. Up to 75% of gastric volvulus cases are associated with para-oesophageal hernias. Occasionally, they can be manipulated endoscopically.
The reassurance: for the common sliding hernia (Type I), these complications are uncommon. The concern: for Types II-IV, watchful waiting requires genuine watching.
Diagnosis
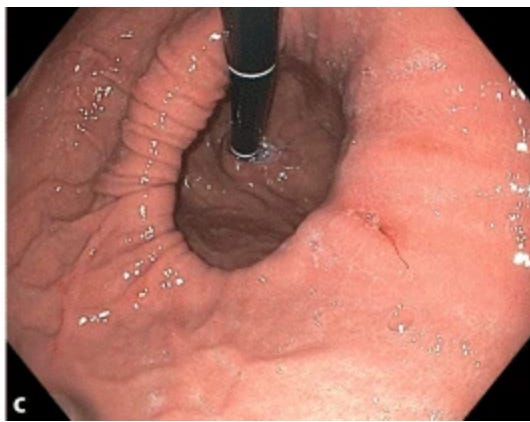
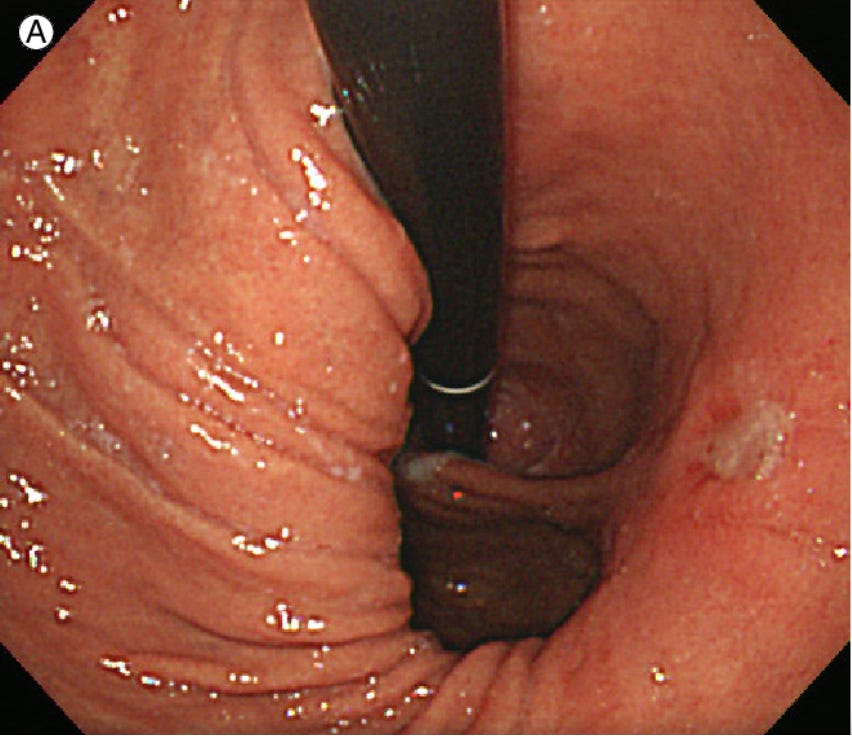
Hiatus hernias are often discovered incidentally…during a gastroscopy performed for something else entirely.
On endoscopy, we look for the gastro-oesophageal junction sitting more than 2cm above the diaphragmatic impression. We also use the Hill classification, viewing the valve from below in retroflexion.
A barium swallow can be useful too…particularly for characterising para-oesophageal hernias and assessing the stomach’s position relative to the diaphragm.

For complex cases, high-resolution manometry offers the most accurate assessment. A meta-analysis of over 5,000 patients found it outperformed both endoscopy and barium studies for diagnostic precision.
But for most people? The gastroscopy that found the hernia is enough.
Management
If you’ve read my previous articles on reflux, you’ll know my approach: lifestyle first, medications when needed, surgery for the select few.
Read here
And once you’ve finished read here
Lifestyle modifications with genuine evidence behind them:
Weight loss - A prospective study of 332 patients showed a dose-response relationship between weight reduction and symptom resolution. Even 5-10% loss can make a meaningful difference.
Head of bed elevation - Elevating by 15-20cm reduces overnight acid exposure. Simple physics: gravity becomes your mate.
Eating patterns - Fast eating, eating beyond fullness, lying down soon after meals….all independently associated with worse reflux.
Medications - Proton pump inhibitors (PPIs) remain the most effective pharmacological option. They block the acid pumps in the stomach lining. For most patients with hiatus hernia-related reflux, they work well.
As mentioned, I’ve written extensively about reflux management here and treatment options here. The principles overlap considerably.
Surgery and endoscopic options
Not everyone needs an operation. But some people do.
Who should be considered for surgery?
Failed medical therapy despite optimisation
Severe erosive oesophagitis (grades C or D)
Large para-oesophageal hernias….especially if symptomatic
Complications: anaemia from Cameron lesions, recurrent aspiration, gastric volvulus
Patient preference (some people simply don’t want lifelong medication)
The operations:
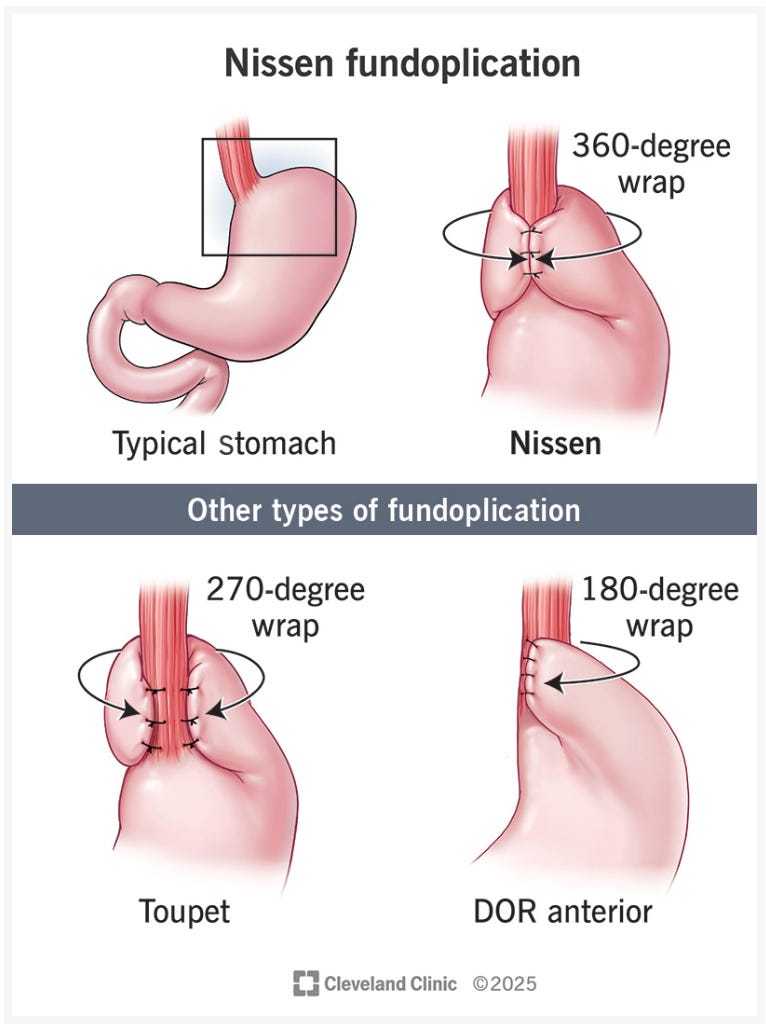
Nissen fundoplication - The stomach’s fundus is wrapped 360° around the lower oesophagus, reinforcing the valve. The gold standard for normal oesophageal motility.
Toupet fundoplication — A 270° partial wrap. Preferred when motility is impaired. A network meta-analysis of 13 randomised trials found Toupet causes less post-operative dysphagia than Nissen, with equivalent reflux control.
Both are now performed laparoscopically (keyhole). Recovery is quicker. Hospital stays average two days.
Risks of surgery:
Modern laparoscopic anti-reflux surgery is safe. A Swedish population study of nearly 9,000 patients found 30-day mortality of just 0.03%. Serious complications occur in around 4% …higher in older patients, lower in younger ones.
The nuisance symptoms are more common: temporary difficulty swallowing, gas-bloating, inability to belch. Most improve with time.
Recurrence:
Rarely, hiatus hernias can come back.
Radiographic recurrence rates vary widely… from 15% to over 30% depending on the study and follow-up duration. Most recurrences appear within the first three years.
However, anatomical recurrence doesn’t always mean symptomatic recurrence. Many patients with a small radiographic recurrence remain perfectly well. Re-operation rates sit around 3-6%.
Larger initial hernias and higher BMI predict higher recurrence risk. Technique matters. A quality improvement study showed standardised surgical protocols reduced recurrence from 21% to 6%.
Endoscopic option?
For those wanting something between pills and surgery, newer endoscopic treatments exist:
TIF (Transoral Incisionless Fundoplication) - Performed through the mouth, no external incisions. Best suited for small hernias (under 2cm). Long-term data shows about 27% of patients remain off PPIs at 8 years. Less invasive, but less durable than surgical fundoplication.
As always….patient selection is everything.
I did say everything in 5 minutes!
A hiatus hernia diagnosis is NOT a disaster. For most people, it’s an incidental finding that explains some symptoms….or explains nothing at all.
Small sliding hernias rarely need more than lifestyle adjustments and occasional medication. Larger or para-oesophageal hernias warrant closer attention. Surgery, when indicated, is safe and effective…though not without trade-offs.
If you’ve been told you have a hiatus hernia, don’t panic. Understand it.
Manage the symptoms. And if those symptoms don’t settle, know that solutions exist.
Struggling with liver or digestive issues that affect your daily life? Invest in your gut health with a private, personalised consultation where I will explore your specific symptoms and develop a targeted treatment plan. Take the first step toward digestive wellness today: https://bucksgastroenterology.co.uk/contact/ (I offer both in person and video consultations!)
References
Kumar D et al. Morphology of the Esophageal Hiatus: Is It Different in 3 Types of Hiatus Hernias? J Neurogastroenterol Motil 2020;26(1):51-60.
Hyun JJ, Bak YT. Clinical Significance of Hiatal Hernia. Gut Liver 2011;5(3):267-277.
Menon S, Trudgill N. Risk factors in the aetiology of hiatus hernia: a meta-analysis. Eur J Gastroenterol Hepatol 2011;23(2):133-8.
Fuchs KH et al. Hiatal Hernias Revisited — A Systematic Review. Life (Basel) 2024;14(9):1145.
Li L et al. Diagnostic accuracy comparison of different modalities for hiatal hernia. J Gastroenterol Hepatol 2020.
Gray DM et al. Cameron lesions in patients with hiatus hernia. Dis Esophagus 2015;28(5):448-452.
Stylopoulos N et al. Paraesophageal Hernias: Operation or Observation? Ann Surg 2002;236(4):492-501.
Singh M et al. Weight loss can lead to resolution of gastroesophageal reflux disease symptoms. Obesity 2013;21(2):284-290.
Network meta-analysis: Dor, Toupet, and Nissen fundoplication long-term outcomes. Surg Endosc 2023.
Maret-Ouda J et al. Mortality from laparoscopic antireflux surgery: a nationwide cohort study. BJS 2017.
SAGES Guidelines: Management of Symptomatic, Asymptomatic, and Recurrent Hiatal Hernia. Surg Endosc 2024;38:4765-4775.
Bell RCW et al. Long-term outcomes of transoral incisionless fundoplication: an 8-year cohort study. Surg Endosc 2019.
General Disclaimer
Please note that the opinions expressed here are those of Dr Hussenbux and do not necessarily reflect the positions of Buckinghamshire Healthcare NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you. Thank you to the amazing photographers from Unsplash where I get most of my images from.
What is the success rate for surgery on an Ehlers Danlos syndrome patient? Many of my surgeries (mostly orthopedic) have failed within 1-2 years due to my faulty collagen.
Please could you do one for Croans. Thank you. Ron Baker