

Is Coffee good for your digestive health?
Your liver's favourite morning ritual

“Doc, why have you always got a coffee in your hand?”
Aaah….coffee.
How much time do you have? Five minutes? Thought so. Let’s talk about it.
Everyone knows about the caffeine benefits. The alertness, the focus, the “don’t speak to me until I’ve had my first cup” energy.
But caffeine is only a fraction of the benefits. Coffee (if bought/sourced correctly) is one of the most chemically complex beverages we consume, and the research behind it has blown me away.
So before you feel guilty about that second cup….read this first.
You can check out my full Substack here
What’s actually in your cup?
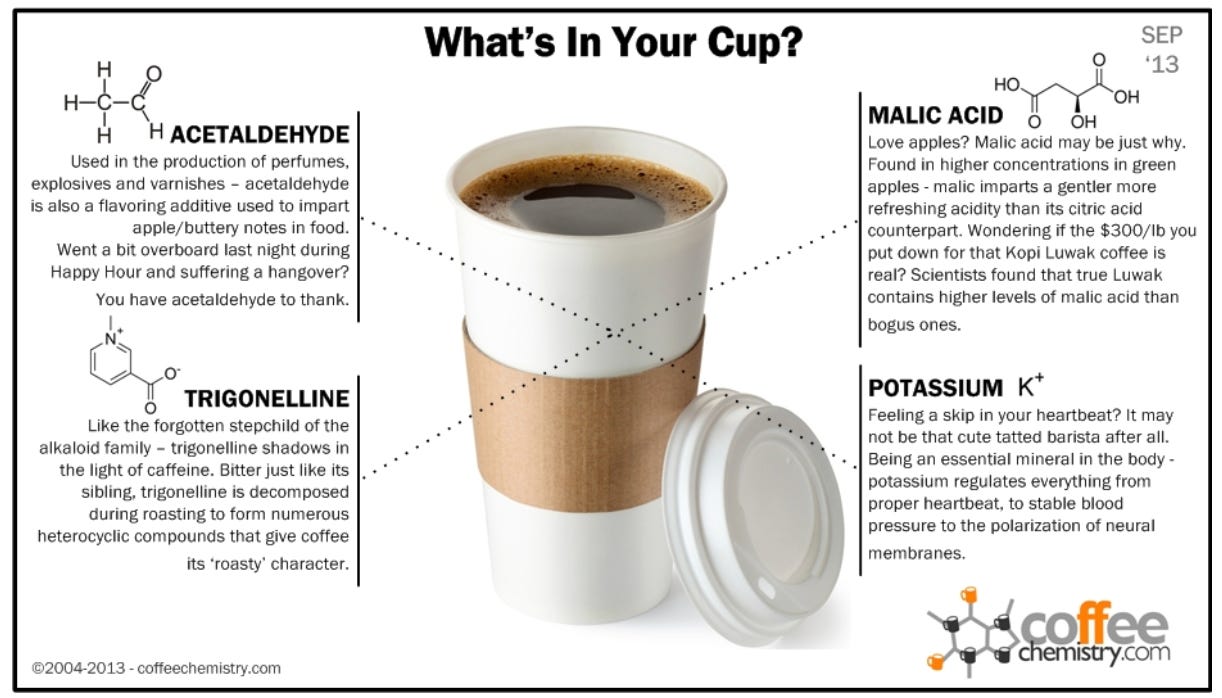
Coffee contains over a thousand bioactive compounds. Here are the ones worth knowing about.
Chlorogenic acids are polyphenols with antioxidant and anti-inflammatory properties. They modulate glucose metabolism and are partially broken down by your gut bacteria into beneficial metabolites.
Melanoidins form during roasting. They act as dietary fibre and prebiotics, promoting the growth of Bifidobacterium species. Coffee as a prebiotic!!
Diterpenes (cafestol and kahweol) are found in unfiltered coffee. Anti-inflammatory. Potentially hepato-protective. But they raise LDL cholesterol. Filtered coffee removes most of these, which becomes relevant later.
Trigonelline converts to niacin (vitamin B3) during roasting and has antibacterial properties in the mouth.
And of course….caffeine! Stimulates gastric acid secretion, promotes colonic motility and keeps your central nervous system alert. (I personally don’t take any caffeine 12 hours before bed).
Coffee and the liver
Strong evidence incoming!
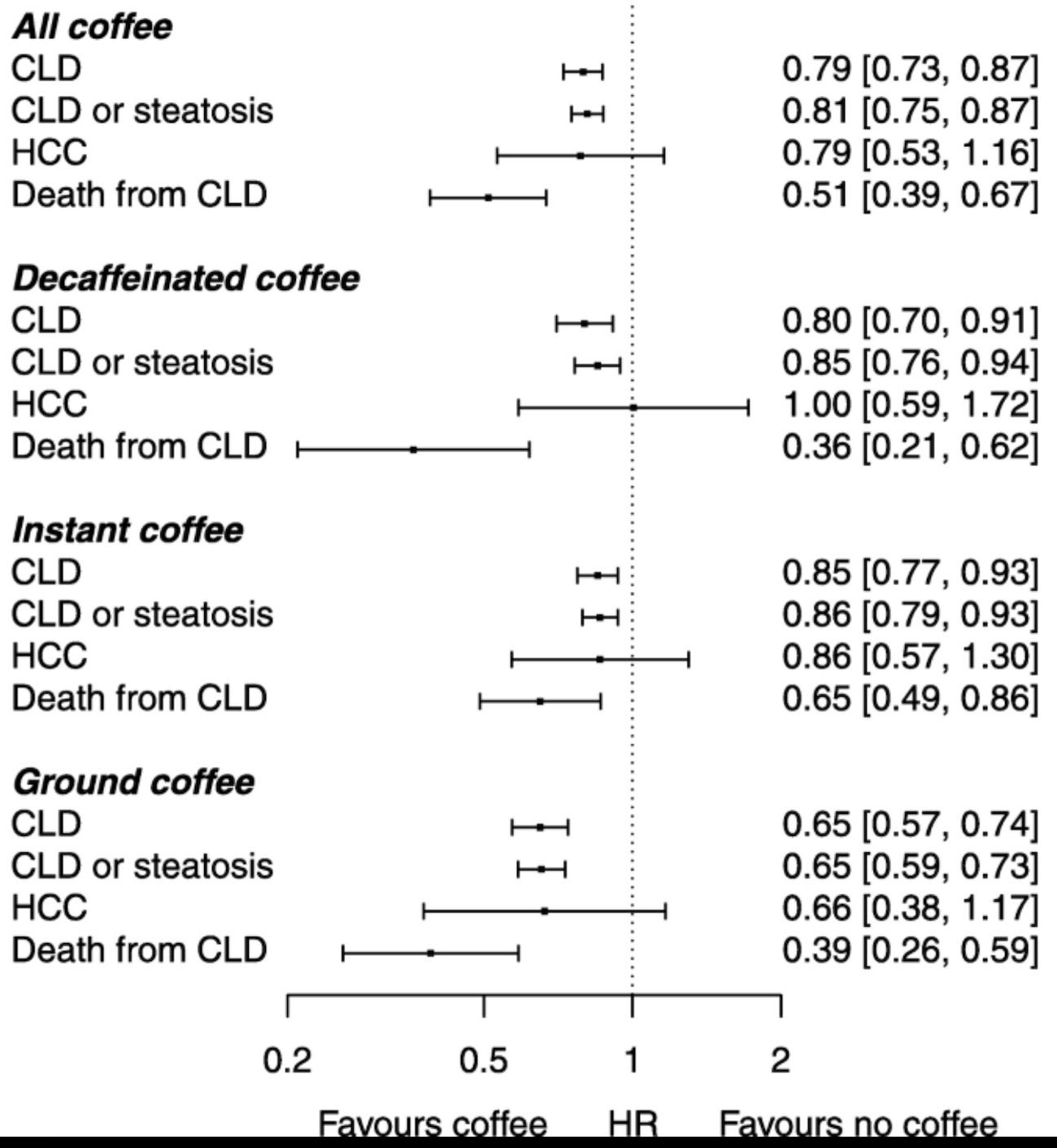
A meta-analysis by Kennedy et al. (BMJ Open, 2016) found that each additional cup of coffee per day was associated with a 22% reduced risk of cirrhosis. Two cups, 44%. The dose-response was linear!
Liver cancer? Pooled data from Bravi et al. (Clinical Gastroenterology and Hepatology, 2017) showed coffee drinkers had roughly 40% lower risk of hepatocellular carcinoma compared with non-drinkers.
I advise most of my cirrhosis/fibrosis patients to have a cup a day.
Even in patients with existing fatty liver disease, coffee consumption has been linked to reduced hepatic fibrosis on elastography (Bambha et al., Liver International, 2014).
The mechanism likely involves reduced hepatic stellate cell activation, the antioxidant effects of chlorogenic acids, and the anti-fibrotic properties of cafestol and kahweol all working together.
But let me be clear. Coffee does not undo the damage of heavy alcohol use or obesity. It modifies risk. It does not reverse established disease. Three lattes do not cancel out three pints. (kind of obvious, but must mention!)
Coffee and your gut
Right. My territory now.
The gastrocolic reflex. Coffee stimulates colonic motor activity within minutes of drinking. A classic study by Rao et al. (European Journal of Gastroenterology and Hepatology, 1998) showed coffee induced colonic contractions in 30% of participants.
That’s comparable to a 1,000 kcal meal. And decaf did it too. Something beyond caffeine is driving this, likely through cholecystokinin (CCK) release and activation of the gastrocolic reflex.
If you’ve ever needed the bathroom shortly after your morning coffee….now you know why!
Reflux. Caffeine stimulates parietal cells, increases gastric acid secretion. You’d assume coffee worsens gastro-oesophageal reflux disease.
But there is some evidence to suggest the contrary!
A meta-analysis by Kim et al. (Journal of Neurogastroenterology and Motility, 2013) found no significant association between coffee and GORD symptoms.
The blanket advice to “cut out coffee for reflux” is not well supported. Individual tolerance varies, but the guilt? Largely undeserved.
HOWEVER, coffee on an empty stomach may still lead to reflux symptoms (through increased gastric acid secretion) so I usually advise to have it with a meal!
The microbiome. Regular coffee drinkers show higher microbial diversity and enrichment in anti-inflammatory taxa. Those melanoidins I mentioned earlier? Prebiotics - they FEED the bacteria you want more of.
Gallstones. Data from the Nurses’ Health Study found regular coffee consumption was associated with reduced gallstone risk in women, likely through enhanced gallbladder contraction and improved bile flow.
Colorectal cancer. Some WEAK evidence suggests an inverse association with colorectal cancer risk (Sartini et al., Nutrients, 2019), though the data here is less robust than for liver cancer. (Pinch of salt).
The practical bit
Two to Three cups per day appears to be the sweet spot across most studies. Roughly 400mg of caffeine. However, one morning cup is also completely fine!
Filtered coffee gives you the liver benefits without the LDL cholesterol rise from diterpenes. A cafetière or espresso? Fine occasionally. But your daily driver is best filtered.
If you have active reflux, experiment. I personally avoid on empty stomach.
Pregnancy: limit to 200mg per day (RCOG guidance). One to two cups depending on strength.
And the most important point. Coffee is not a treatment. It is a modifier of risk. It sits alongside a good diet, not instead of one.
You can’t espresso your way out of a poor lifestyle.

There you go
A simple drink. Centuries old. Protecting your liver, feeding your microbiome, moving your colon, and tasting wonderful while doing it.
The guilt around coffee has always puzzled me.
The data says relax.
Pour yourself another cup.
Struggling with liver or digestive issues that affect your daily life? Invest in your gut health with a private, personalised consultation where I will explore your specific symptoms and develop a targeted treatment plan. Take the first step toward digestive wellness today: https://bucksgastroenterology.co.uk/book-an-appointment/ (I offer both in person and video consultations!)
You can check out my full Substack here
References
Kennedy OJ, et al. Systematic review with meta-analysis: coffee consumption and the risk of cirrhosis. BMJ Open. 2016;6(5):e009497.
Bravi F, et al. Coffee and the risk of hepatocellular carcinoma and chronic liver disease: a systematic review and meta-analysis of prospective studies. Clin Gastroenterol Hepatol. 2017;15(9):1360-1368.
Bambha K, et al. Coffee consumption in NAFLD patients with lower insulin resistance is associated with lower risk of severe fibrosis. Liver Int. 2014;34(8):1250-1258.
Rao SS, et al. Is coffee a colonic stimulant? Eur J Gastroenterol Hepatol. 1998;10(2):113-118.
Kim J, et al. Association between coffee intake and gastroesophageal reflux disease: a meta-analysis. J Neurogastroenterol Motil. 2013;19(4):524-531.
Sartini M, et al. Coffee consumption and risk of colorectal cancer: a systematic review and meta-analysis. Nutrients. 2019;11(11):2553.
General Disclaimer
Please note that the opinions expressed here are those of Dr Hussenbux and do not necessarily reflect the positions of Buckinghamshire Healthcare NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you. Thank you to the amazing photographers from Unsplash where I get most of my images from.
I was just starting a coffee as I read this. .... very happy now.
Dr Arif, your posts are so brilliant - really informative, I trust all the information and research you do and they are also really funny. The focus on the gut is just ace for me and it is the centre of everything along with the brain. Your posts brighten up my day. Just like a good cup of coffee. Thank you.