

A Patient's Guide to Ulcerative Colitis
What it is, how we treat it, and what comes next

Mr K was thirty-two. Fit. A new dad.
He came to clinic with four weeks of blood in his stools, urgency he could not explain to his colleagues, and 7kg lost from a frame that did not have weight to spare.
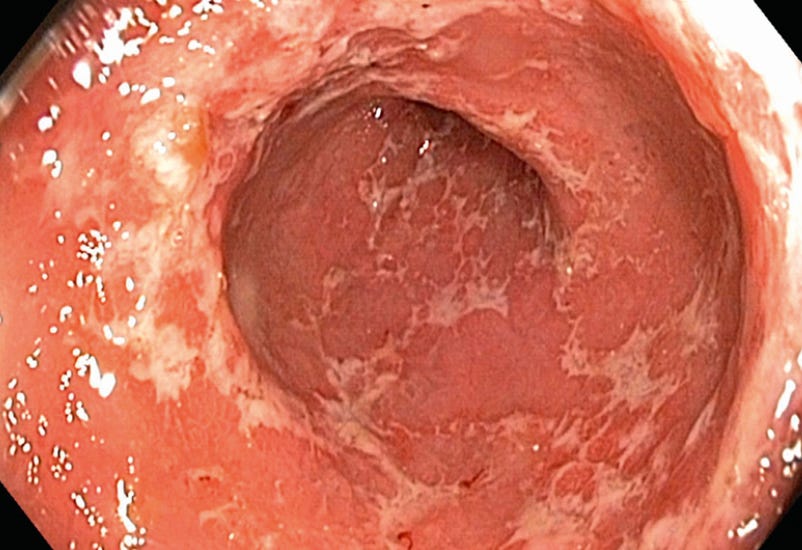
The flexible sigmoidoscopy that afternoon told the story I half expected.
Severe ulceration. Friable mucosa. The vascular pattern gone.
We started intravenous steroids. Within days, the bleeding eased. Within weeks, with the addition of a biological drug called infliximab, he was back on the play mat with his daughter.
This is ulcerative colitis. A condition that is far better understood than it used to be.
Disclaimer: This is general education, not personal medical advice. If you have rectal bleeding, weight loss, or a change in bowel habit for more than a couple of weeks, please see your healthcare professional. Don’t sit on it.
What is Ulcerative Colitis?
Ulcerative colitis (UC) is an autoimmune condition.
Your immune system, which should defend you, instead turns on the lining of your large bowel.
It almost always starts distally, in the rectum, and tends to extend proximally over time. Some people have proctitis only. Others have left-sided colitis. A smaller group develop pancolitis, where the whole colon is involved.
The inflammation is continuous, not patchy. It sits in the mucosa (the inner lining); not deep through the bowel wall. That distinction is what separates UC from its cousin, Crohn’s disease.
The UK has one of the highest rates of UC in the world. Recent primary care data put the prevalence at around 570 per 100,000. The numbers are still climbing.
Symptoms to Watch For
The classic story is bloody diarrhoea. The full picture is broader.
Urgency. When you gotta go you can’t wait.
Tenesmus. The frustrating feeling of needing to go, even when you have just been.
Abdominal pain…usually a later sign indicating more severe disease.
Weight loss and fatigue. Easy to dismiss (as was for Mr K).
Nocturnal symptoms. Waking from sleep to open your bowels is never normal.
And then the signs outside the gut. Joint pain. Painful red eyes (episcleritis, uveitis). Tender skin nodules (erythema nodosum). Painful skin ulcers (pyoderma gangrenosum). UC can show up in places that have nothing obvious to do with the colon.
If your bowels have changed for more than a couple of weeks, and especially if there is blood, please get checked.

Diagnosis
The gold standard is colonoscopy with biopsies.
We look for the endoscopic features Mr K had: loss of the normal vascular pattern, granularity, friability (mucosa that bleeds at the lightest touch), and ulceration. The inflammation runs continuously from the rectum upward. No skip lesions.
Biopsies confirm chronic inflammation in the mucosa and (hopefully) rule out infection or Crohn’s.
Treatment: The Medical Side
Steroids are for induction, not maintenance.
The original randomised controlled trial by Truelove and Witts (BMJ, 1955) is a beautiful piece of medical history. 210 patients. Cortisone or placebo. Remission in 41% versus 16%. Seventy years on, steroids still pull most flares back from the brink. But long-term steroids cause harm. They are a bridge, not a destination.
Mesalazine (5-ASA) is the workhorse for mild to moderate disease. The ASCEND trials showed that 4.8 g/day produced better mucosal healing than 2.4 g/day in moderately active disease. Oral plus rectal preparations work better than oral alone for left-sided disease.
Biological and small-molecule drugs are where UC care has changed in the last twenty years. They work in different ways. The right drug depends on the patient.
A whistle-stop tour:
Infliximab and adalimumab block tumour necrosis factor alpha (anti-TNF). The ACT 1 and ACT 2 trials (Rutgeerts, NEJM, 2005) and the ULTRA trials established their place.
Vedolizumab blocks gut-specific α4β7 integrin; stopping inflammatory cells from trafficking into the bowel. The GEMINI 1 trial (Feagan, NEJM, 2013) confirmed it works.
Tofacitinib and upadacitinib are oral JAK inhibitors. The OCTAVE programme (Sandborn, NEJM, 2017) and the U-ACHIEVE/U-ACCOMPLISH trials (Danese, Lancet, 2022) showed both can induce and maintain remission, including in patients who have already failed biologicals.
There is no single best drug. Your gastroenterologist will work with you to match the medicine to your disease, your previous responses, and your circumstances.
Modern UC care is genuinely tailored.
Treatment: When Surgery is the Right Answer
For severe disease that does not respond to medication, or for dysplasia (pre-cancerous changes), surgery can be lifesaving.
The classic emergency operation is a sub-total colectomy with end ileostomy (a stoma). The diseased organ comes out, and the disease comes out with it. Many patients later go on to have ileoanal pouch surgery. Many live well with a stoma long-term.
Modern stoma care is excellent. People run marathons. People raise families. People go on holiday and forget about it for hours at a time.

The Long View: Cancer Surveillance and Living Well
Long-standing UC carries an increased risk of colorectal cancer.
That is why surveillance colonoscopy, usually starting eight to ten years after diagnosis, is part of every patient’s plan. Frequency depends on extent of disease, family history, primary sclerosing cholangitis, and previous findings. The BSG (Lamb, 2019), ECCO (Magro, 2017) and AGA all recommend it.
UC is not a condition you manage alone.
A dietitian helps with nutrition during flares and recovery. An IBD nurse becomes a lifeline. A gastroenterologist who knows you well makes everything easier. Surgeons, mental health support, the wider multidisciplinary team. The BSG guidelines lay this out for good reason.
In Summary
Mr K is now in remission. Back to work. Back to his daughter. Back to the quiet, ordinary life he had before.
His colon is still his colon. His disease is managed, not cured.
UC is lifelong. But it is no longer the condition it was in 1955. We have evidence. We have biologicals. We have surgery when we need it. And we have time.
If anything you have read here rings a bell, please see your GP. Early diagnosis changes everything.
Struggling with liver or digestive issues that affect your daily life? Invest in your gut health with a private, personalised consultation where I will explore your specific symptoms and develop a targeted treatment plan. Take the first step toward digestive wellness today: https://bucksgastroenterology.co.uk/book-an-appointment/ (I offer both in person and video consultations!)
You can check out my full Substack here
References
Truelove SC, Witts LJ. Cortisone in ulcerative colitis: final report on a therapeutic trial. BMJ. 1955;2(4947):1041–1048.
Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. NEJM. 2005;353(23):2462–2476.
Reinisch W, Sandborn WJ, Hommes DW, et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis (ULTRA 1). Gut. 2011;60(6):780–787.
Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis (ULTRA 2). Gastroenterology. 2012;142(2):257–265.
Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis (GEMINI 1). NEJM. 2013;369(8):699–710.
Sandborn WJ, Su C, Sands BE, et al. Tofacitinib as induction and maintenance therapy for ulcerative colitis (OCTAVE). NEJM. 2017;376(18):1723–1736.
Danese S, Vermeire S, Zhou W, et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis (U-ACHIEVE / U-ACCOMPLISH). Lancet. 2022;399(10341):2113–2128.
Hanauer SB, Sandborn WJ, Kornbluth A, et al. Delayed-release oral mesalamine at 4.8 g/day for moderately active ulcerative colitis (ASCEND II). Am J Gastroenterol. 2005;100(11):2478–2485.
Sandborn WJ, Regula J, Feagan BG, et al. Delayed-release oral mesalamine 4.8 g/day is effective in moderately active ulcerative colitis (ASCEND III). Gastroenterology. 2009;137(6):1934–1943.
Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526–535.
Jess T, Rungoe C, Peyrin-Biroulet L. Risk of colorectal cancer in patients with ulcerative colitis: a meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10(6):639–645.
Travis SPL, Schnell D, Krzeski P, et al. Developing an instrument to assess the endoscopic severity of ulcerative colitis: the UCEIS. Gut. 2012;61(4):535–542.
Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106.
Magro F, Gionchetti P, Eliakim R, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. J Crohns Colitis. 2017;11(6):649–670.
King D, Reulen RC, Thomas T, et al. Changing patterns in the epidemiology and outcomes of inflammatory bowel disease in the United Kingdom: 2000–2018. Aliment Pharmacol Ther. 2020;51(10):922–934.
Hsu SH, et al. Colorectal cancer risk in ulcerative colitis: an updated population-based systematic review and meta-analysis. eClinicalMedicine. 2025;83:103210.
General Disclaimer
Please note that the opinions expressed here are those of Dr Hussenbux and do not necessarily reflect the positions of Buckinghamshire Healthcare NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you. Thank you to the amazing photographers from Unsplash where I get most of my images from.
So good to have all of these things explained so well - you have a true gift of communication! Thank you 🙏
Nice simple overview. Thanks. Don't forget primary sclerosing cholangitis and thromboembolic.