

The only colonoscopy guide you need
From a doctor who does this every day

Your doctor just said four words that sent your imagination into overdrive.
“You need a colonoscopy.”
A tube. Up where??
Take a breath and sit down!
Let me walk you through this…step by step, plainly, without the fuss.
I do this procedure multiple times per week.
And I can tell you, with complete confidence, that the procedure is nowhere near as terrifying as the mind makes it.
Here is what you need to know.
You can check out my full Substack here
Can’t be bothered to read? I got you with the video version!
What is a colonoscopy?
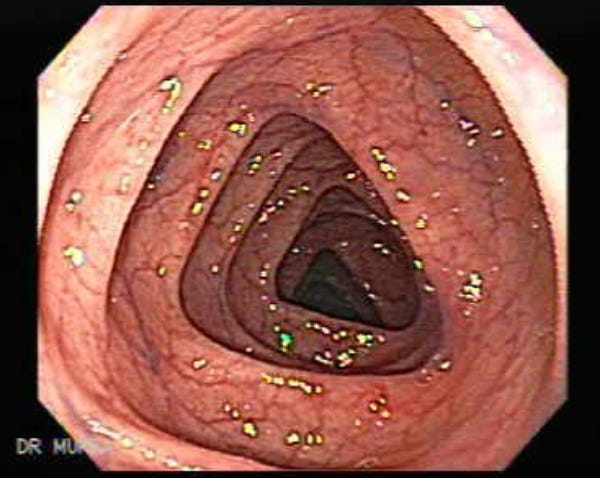
A colonoscopy is an examination of the lining of your large bowel (the colon and rectum) using a long, flexible camera called a colonoscope.
Think of it as a detailed map of your gut.
The scope is roughly the width of a finger. It travels the full length of the colon, all 1.5 metres of it, transmitting live images to a screen. We look for inflammation, bleeding sources, abnormal tissue, and polyps (more on those in a moment).
It sounds dramatic but it rarely is.
Why might you need one?
There are a handful of common reasons your doctor might refer you. All of them deserve to be taken seriously.
Rectal bleeding. Blood in the stool (or on the paper) is never something to wave away. Most causes are benign: haemorrhoids, a small fissure. But the bowel is not somewhere we guess.
A change in bowel habits. Persistent loose stools, constipation, or a change in consistency lasting more than a few weeks. Your bowel is usually consistent. When it isn’t, we want to know why.
Family history of bowel cancer. A close relative diagnosed with colorectal cancer, particularly before age 60, meaningfully raises your risk. Screening in this context isn’t precautionary. It should be discussed with a specialist.
A concerning finding on CT. Sometimes imaging picks up something in the colon that needs a proper look. A colonoscopy gives us the definitive answer.
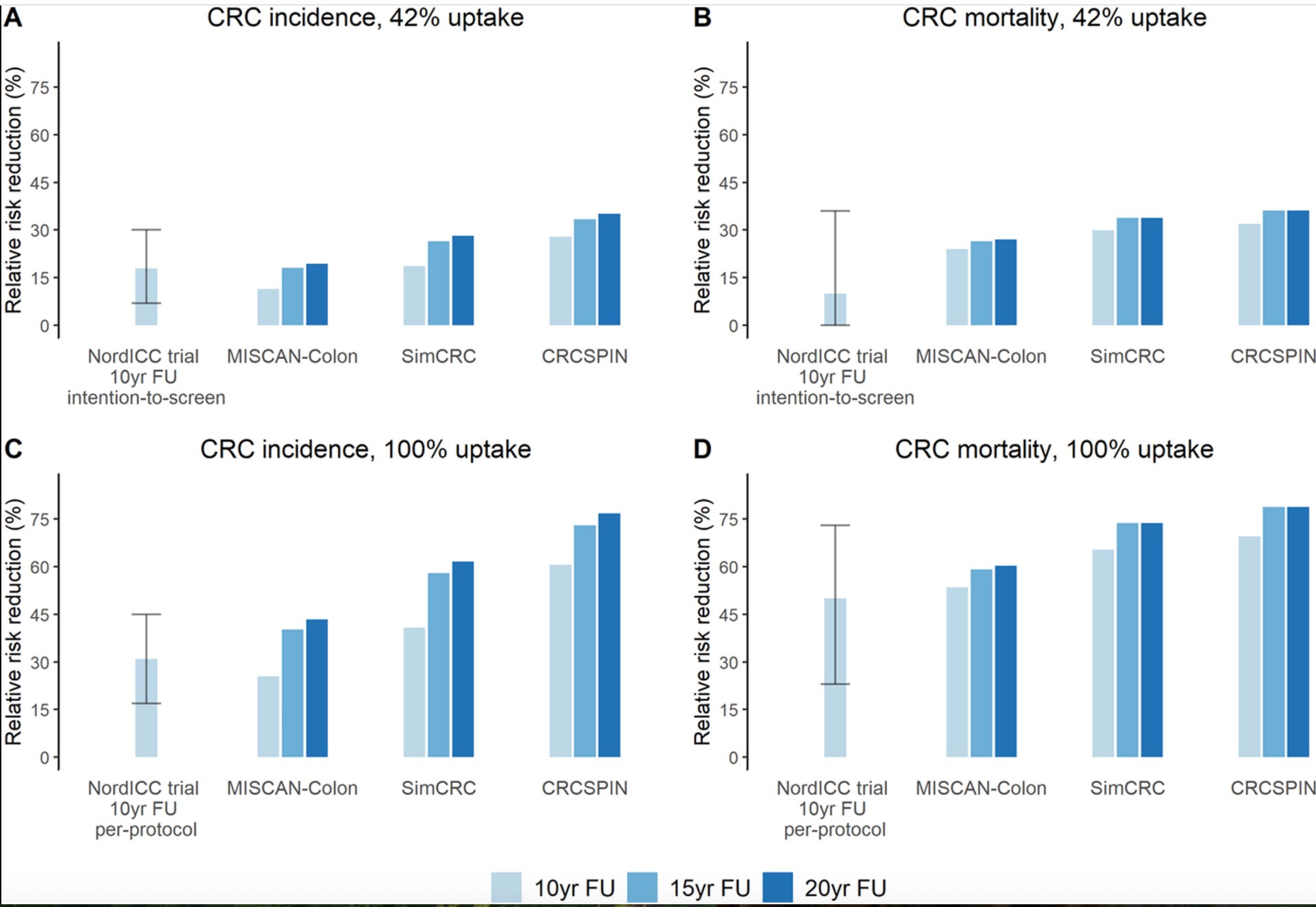
Screening. Bowel cancer is the UK’s second biggest cancer killer. The NordICC trial, the largest randomised controlled trial of screening colonoscopy ever conducted, found that among those who actually underwent the procedure, the risk of developing bowel cancer fell by 31%, and the risk of dying from it fell by 50%.
That is not a modest number.
Is it safe?
Yes. Clearly and unequivocally yes.
Colonoscopy is one of the most commonly performed procedures in gastroenterology, and one of the most rigorously studied. Serious complications are rare.
Perforation (a small tear in the bowel wall) occurs in approximately 1 in every 2000 diagnostic procedures. Significant bleeding after large polyp removal happens in around 1 in 100 cases. It almost always settles without intervention. Mortality directly attributable to colonoscopy is approximately 3 in every 100,000 procedures.
For context: you face more risk on the drive to the hospital.
The small risk of the procedure is real. The risk of missing bowel cancer is far greater. The calculation, weighed honestly, is not a close one.
What actually happens?
The bowel prep
To see the bowel wall clearly, it must be empty. Completely.
The day before your procedure, you’ll drink a bowel preparation solution: a laxative that flushes the colon entirely clean. These agents work primarily by drawing water into the bowel (osmotic laxatives), stimulating it to contract and clear its contents. The result is….vigorous to say the least!
It is not pleasant. I won’t pretend otherwise.
But here’s what the evidence tells us: split-dose preparation (half the night before, half the morning of) is significantly better tolerated and significantly more effective than drinking it all at once.
A meta-analysis of 47 randomised controlled trials confirmed split-dosing produces a cleaner bowel, and patients are nearly twice as likely to say they’d do it again.
Follow the instructions exactly. A clean colon means a safe, thorough procedure. Poor preparation is the single most common reason colonoscopies miss things that matter.
Do the prep properly please!

On the day
You’ll arrive fasted. A small cannula goes into your arm. You’ll meet the nursing team, sign a consent form, and be walked through what to expect.
For sedation, you have options. The right choice depends on you:
Gas and air (Entonox): Inhaled through a mouthpiece. Takes the edge off. Keeps you awake but calm. Main benefit is you won’t need anyone to drop or pick you up; you can get on with your day straight after!
Intravenous sedation (midazolam + fentanyl): The most common approach. You’ll be drowsy, deeply relaxed, and most patients remember very little. I perform the vast majority of my colonoscopy with this approach.
I offer this procedure at The Chiltern Hospital and The Royal Buckinghamshire Hospital
Propofol sedation with an anaesthetist: A deeper level of sedation, sometimes offered privately or for more complex cases. Recovery is faster. Patient satisfaction scores are slightly higher. I offer propofol endoscopy at The Spire Thames Valley Hospital. To book a consultation click here
All three are safe. All three are well-established. There is no “best”. Only what’s right for you.
The procedure
You’ll lie on your left side. I / the endoscopist pass the colonoscope gently through the rectum and advances it slowly, carefully, around the full length of the colon, using water to see where I need to go next.
The procedure itself usually takes 20 to 40 minutes.
You may feel some pressure or bloating as the scope navigates the corners of the colon. That’s normal. Discomfort is common. Pain is not.
On the way back out, I examine the mucosal lining with careful attention. Biopsies can be taken immediately. Abnormalities are photographed and documented. And if there are polyps….
Polyps. Should I worry?
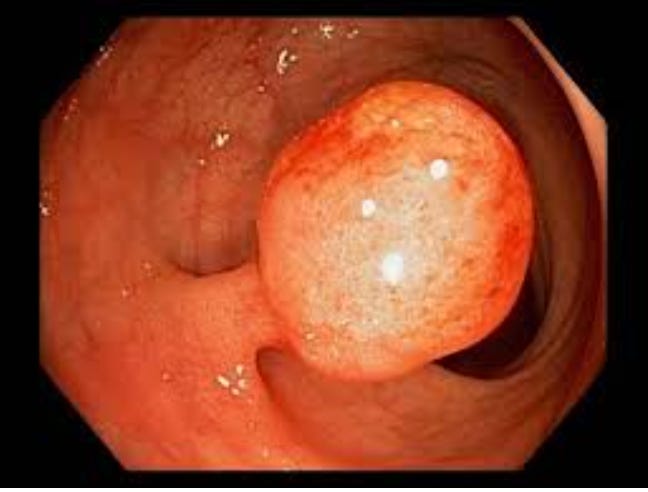
Polyps are small growths on the bowel lining. Common. Most are entirely harmless.
Some, however, are adenomas: precancerous lesions that, left undiscovered and undisturbed over years, may develop into cancer. Finding them is good news, not bad. It means the colonoscopy did exactly what it was meant to do.
If a polyp is found, it is almost always removed on the spot. A painless process called polypectomy, using a small wire loop with or without heat. You won’t feel it.
A landmark study in the New England Journal of Medicine (314,872 colonoscopies, 136 endoscopists) found that for every 1% increase in adenoma detection rate, the risk of interval bowel cancer fell by 3%.⁵
After: tea and biscuits
Once it’s done, you’ll be moved to a comfortable recovery area.
Tea. Biscuits. A moment to breathe.
The sedation takes one to two hours to fully clear, so a responsible adult needs to take you home. No driving and no alcohol. No important decisions for the rest of the day.
If biopsies were taken or polyps removed, results typically come back within a few weeks. The endoscopist will usually give you a verbal summary before you leave, so you won’t walk out wondering.
Most patients report the same thing afterwards: it was nothing like I expected. The anticipation is always worse than the procedure itself. Always.
Watch: a short video walkthrough
I’ve put together a short video explaining the procedure. Worth watching before your appointment.
▶️ Watch here
One final thought
Bowel cancer caught early is one of the most treatable cancers we have. Five-year survival for localised disease exceeds 90%. Caught late, the picture changes profoundly.
A colonoscopy is not the best day out. No one is claiming it is.
But it may be the most important appointment you keep this year.
Don’t let the fear of the procedure eclipse the far greater risk of missing something that matters.
The camera goes in. The answers come out.
That is worth everything.
If you enjoyed this article check out my Substack here
Struggling with liver or digestive issues that affect your daily life? Invest in your gut health with a private, personalised consultation where I will explore your specific symptoms and develop a targeted treatment plan. Take the first step toward digestive wellness today: https://bucksgastroenterology.co.uk/contact/ (I offer both in person and video consultations!)
References
Bretthauer M, et al. Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. N Engl J Med. 2022;387:1547–1556.
Reumkens A, et al. Post-Colonoscopy Complications: A Systematic Review, Time Trends, and Meta-Analysis of Population-Based Studies. Am J Gastroenterol. 2016;111:1092–1101.
Martel M, et al. Split-Dose Preparations Are Superior to Day-Before Bowel Cleansing Regimens: A Meta-analysis. Gastroenterology. 2015;149:79–88.
Vargo JJ, et al. Propofol versus midazolam/opioid for colonoscopy sedation: a systematic review and meta-analysis. Gastrointest Endosc. 2020;91:786–793.
Corley DA, et al. Adenoma Detection Rate and Risk of Colorectal Cancer and Death. N Engl J Med. 2014;370:1298–1306.
Siegel RL, et al. Colorectal Cancer Statistics, 2026. CA Cancer J Clin. 2026.
General Disclaimer
Please note that the opinions expressed here are those of Dr Hussenbux and do not necessarily reflect the positions of Buckinghamshire Healthcare NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you. Thank you to the amazing photographers from Unsplash where I get most of my images from.
Having had 2 I can confirm that the worst part is the bowel prep. Also staff are so professional and caring
Dr H does a great colonoscopy..lay back and relax..shut youer eyes, sleep for a short time..the Tea and Biscuits...To be honest the pre prepartion is the interesting bit !